What the retina and macula are
The retina is a thin, light-sensitive layer lining the inside back of the eye, about the thickness of a business card. Made of light-sensing cells (photoreceptors) and nerve cells, it processes incoming light and sends it to the brain through the optic nerve. In short, the retina is the eye's seeing centre.
There are two main light cells: rods handle low-light and peripheral vision, while cones work in bright light and are responsible for colour and sharp, central vision.
The macula
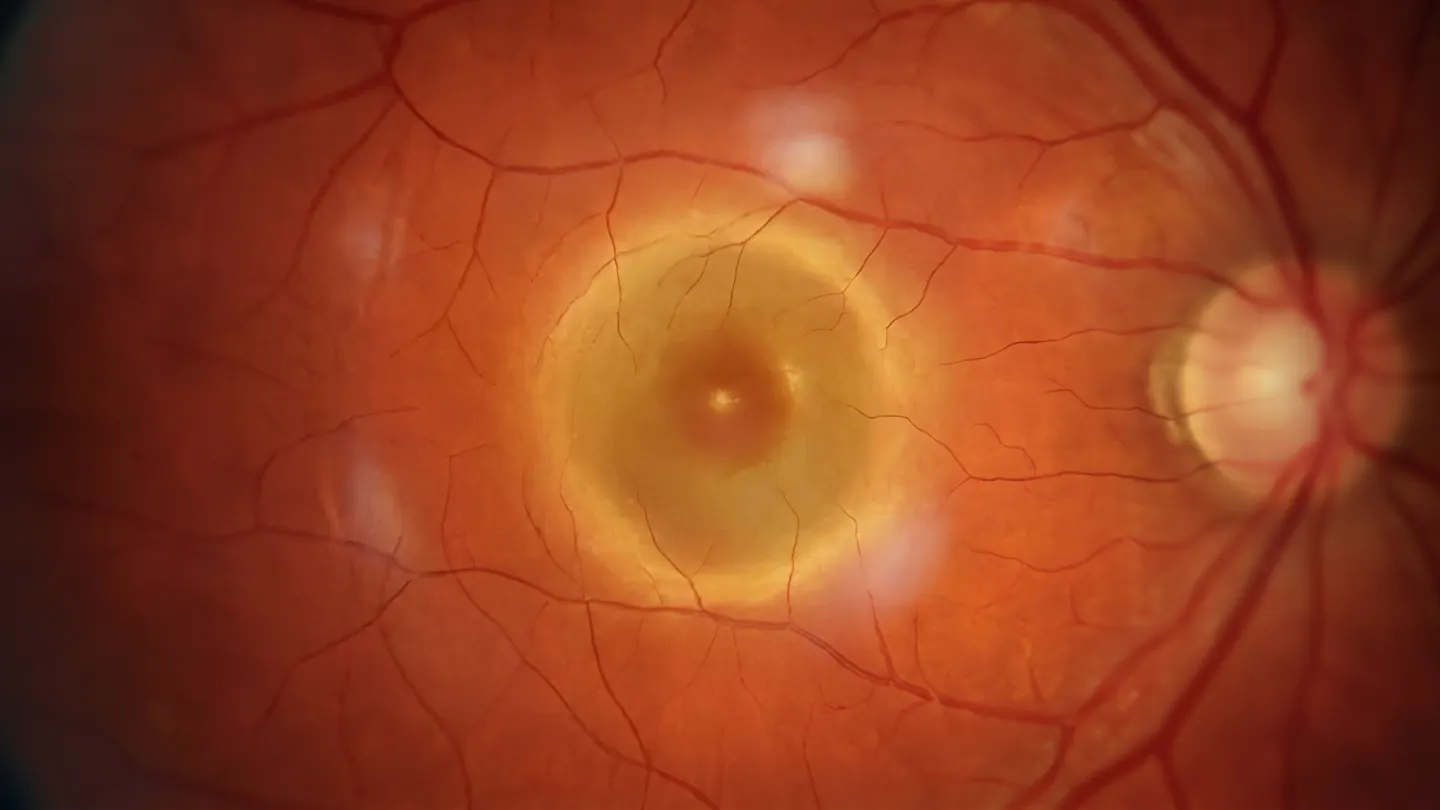
The macula sits at the very centre of the retina and is responsible for central vision. It makes sharp, detailed sight possible and is where light is focused. The fovea, at its very middle, is where the sharpest vision occurs. It takes its name, the yellow spot, from its dense pigment.
The macula is highly intolerant of oxygen deprivation. When the body's or the retina's oxidant-antioxidant balance is disturbed, the macula suffers and various conditions can arise. As I always tell my patients: a healthy retina lives in a healthy body.
- Fovea
- The very centre of the macula; the eye's point of sharpest vision.
- Photoreceptors
- The rod and cone cells that turn light into nerve signals.
- Vitreous
- The clear gel filling the eye, sitting in front of the retina.
Symptoms and when to seek care
Retina conditions often progress quietly. When any of the following appears, seeing an eye doctor without delay is one of the biggest factors in how much vision can be preserved.
- A sudden burst of many new floaters
- Repeating flashes of light, especially at the edge of your vision
- A grey or dark curtain creeping in from one side
- Straight lines that look wavy, or a blank spot in the centre
- A sudden drop in vision in one eye
- Objects appearing larger, smaller or distorted
Sudden flashes, a curtain descending over your vision, or a sudden loss of sight can signal a retinal tear or detachment and warrant a same-day assessment.
How we examine the retina
Accurate diagnosis usually rests on a detailed examination, often with the pupil dilated, together with modern imaging. These methods can reveal subtle changes before vision is noticeably affected.
-
Optical Coherence Tomography
OCTProduces cross-sectional images of the retinal layers, almost like taking a tissue sample. It reveals fluid, swelling and the smallest changes in the macula. It does not touch the eye.
-
OCT Angiography
OCTAMaps the retinal vessels without any dye, by measuring how light reflects off moving blood cells. Especially valuable in vascular conditions affecting the macula.
-
Fluorescein Angiography
FFAUses an injected fluorescein dye to image the retinal vessels, clearly showing leakage, blockages and abnormal vessels.
-
Fundus Examination
FundoscopyDirect examination of the retina, optic nerve and macula with a special lens and light; the most fundamental step in assessing the retina.
-
Amsler Grid
A simple grid test that reveals distortion in central vision. Patients can use it at home to catch early signs.
-
Electrophysiology
ERG / VEPMeasures the electrical activity of retinal cells and the visual pathways. Used in diagnosing inherited conditions such as retinitis pigmentosa.
Retina conditions I focus on
Below is a brief overview of the main conditions affecting the retina and macula. Each is for information only; diagnosis and treatment vary from person to person.
Diabetic Retinopathy Damage to the retinal vessels from high blood sugar; one of the most common causes of vision loss in adults.
Symptoms: Blurred vision, Floaters, Dark areas in the field, Sudden vision loss
Diabetes affects the small blood vessels and also causes nerve damage (neurodegeneration). Rich in both nerve and vascular cells, the retina is the tissue most affected by this disease.
The early (non-proliferative) stage usually has no symptoms; microaneurysms and small haemorrhages form in the vessels. In the advanced (proliferative) stage, abnormal new vessels grow that can bleed and pull, leading to severe vision loss and retinal detachment. When fluid collects in the macula (diabetic macular oedema), central vision drops markedly.
Treatment rests on controlling blood sugar, blood pressure and cholesterol; laser, intravitreal anti-VEGF injections and, in advanced cases, vitrectomy are used as needed. Everyone diagnosed with diabetes should have a retinal exam at least once a year.
Age-Related Macular Degeneration (AMD) Loss of central vision from damage to the macula in people over 55; the best-known retinal disease.
Symptoms: A spot or gap in the centre, Straight lines looking wavy, Faded colours
The dry type is the most common form (about 80% of patients) and progresses slowly. Deposits called drusen form under the retina, the macula thins and central vision gradually declines.
The wet type is less common but faster and more serious. Abnormal vessels growing under the retina leak and bleed; left untreated they can cause permanent damage.
In the wet type, intravitreal anti-VEGF injections suppress the growth of abnormal vessels. In the dry type, certain vitamin and mineral supplements (AREDS) have been shown to slow progression. Quitting smoking and eating well reduce the risk.
Retinal Detachment The retina separating from the supporting tissue beneath it, like wallpaper peeling off a wall. An emergency.
Symptoms: Sudden flashes of light, Many floaters, A curtain over the vision
From the moment the retina starts to separate, nerve cells begin to be lost; the detached area loses its blood supply and oxygen. Left untreated it leads to permanent vision loss.
It usually develops after a retinal tear, when intraocular fluid seeps beneath the retina. High myopia, eye trauma, previous eye surgery and diabetic retinopathy all raise the risk.
In early, limited cases the area around the tear can be secured with laser or cryotherapy. In advanced cases the retina is repositioned with surgery such as vitrectomy or scleral buckling. Treatment should begin as soon as possible.
Retinal Tear A tear caused by the vitreous pulling on the retina. Left untreated it can progress to detachment.
Symptoms: Sudden flashes, New floaters, Shadowing at the edge
With age the vitreous gel shrinks, sticks to the retina and tugs on it; this traction can create a tear. High myopia, trauma and previous eye surgery raise the risk.
Seeking care as soon as symptoms appear is critical. Laser (photocoagulation) or cryotherapy applied around the tear can prevent fluid from seeping underneath and stop a detachment from developing.
Retinal Vascular Occlusions Blockage of a retinal vein or artery; can cause sudden, painless vision loss.
Symptoms: Sudden painless vision loss, A dark area in the field, Blurred vision
Nerve cells are very intolerant of oxygen loss; if a blockage is not relieved quickly, permanent retinal damage follows. Vein occlusions (central CRVO, branch BRVO) cause leakage and oedema; artery occlusions (CRAO, BRAO) cause a sudden loss of blood flow.
The main risk factors are high blood pressure, diabetes, high cholesterol, smoking and arteriosclerosis. Treatment involves controlling the underlying vascular disease, anti-VEGF or corticosteroid injections and laser. Artery occlusions need emergency assessment.
Epiretinal Membrane (Macular Pucker) A thin membrane forming on the macular surface that can distort vision over time.
Symptoms: Distorted or wavy vision, Reduced central vision
It usually develops with age or after minor damage to the retina. Thin at first, it may cause no symptoms; over time it tugs on the macula, distorting its shape, or thickens and reduces vision.
Mild cases can be monitored. With significant vision loss, peeling the membrane during vitrectomy aims to improve vision; it is surgery that requires experience.
Macular Hole A small hole at the centre of the macula that can seriously affect central vision.
Symptoms: A spot in the centre, Bending of straight lines, Difficulty seeing detail
It usually forms when the vitreous pulls on the macula with age; trauma and other retinal diseases can also cause it. It progresses through three stages, and central vision loss grows as the hole enlarges.
The most common treatment is vitrectomy: the vitreous is removed and a gas bubble is placed inside the eye to help the hole close. Head positioning afterwards may matter; visual recovery can take a few months.
Hypertensive Retinopathy Narrowing, hardening and damage of the retinal vessels caused by high blood pressure.
Symptoms: Blurred vision, Dark spots in the field, Vision loss in advanced stages
High blood pressure narrows and hardens the retinal vessels; in advanced stages bleeding, fluid leakage and swelling of the optic nerve (papilloedema) can appear. It is usually classified into four stages.
The first step in treatment is bringing blood pressure under control. Because it often causes no symptoms, regular eye exams are important; advanced cases may need laser or injections.
Retinitis Pigmentosa An inherited, progressive disease marked by the slow loss of light-sensitive cells.
Symptoms: Night blindness, Tunnel vision, Narrowing visual field
Because the rod cells are affected first, the earliest sign is usually night blindness. As it progresses, peripheral vision is lost and tunnel vision develops; in late stages central vision can be affected too.
There is no definitive cure yet; care aims to slow progression and preserve quality of life. Research continues in areas such as gene therapy, stem cells and the bionic eye. People with a family history should have regular check-ups.
Vitreous Conditions Age-related changes in the clear gel that fills the eye: separation, floaters and bleeding.
Symptoms: Floaters, Flashes of light, Sudden blurring
With age the vitreous shrinks and separates from the retina (vitreous detachment). This is usually harmless, but it can pull on the retina and cause a tear or detachment. Bleeding into the vitreous (vitreous haemorrhage) can cause sudden vision loss.
Mild floaters usually need no treatment. When the vitreous pulls on the macula (vitreomacular traction) or there is heavy bleeding, an intravitreal injection or vitrectomy may be considered.
Treatment approaches
Care for retinal disease may involve monitoring, intravitreal injections, laser or surgery. Which approach fits is something we decide together, going through the findings and the options.
Because of the blood-retina barrier, many medicines given by mouth or vein cannot reach the retina well, and eye drops cannot fully penetrate to the back of the eye. So in retinal and macular disease the medication is often delivered directly inside the eye.
The results of surgical and interventional procedures may vary from person to person.
Protecting your retinal health
Anything that harms the body can affect vision too. A few simple habits help protect retinal health.
A balanced diet
Leafy greens and fish rich in lutein, zeaxanthin and omega-3 support the retina against oxidative stress.
Regular eye exams
Retinal disease may give no early signs. A yearly exam matters especially over 40 and for those at risk.
Control diabetes, blood pressure, cholesterol
Keeping these in check is decisive in preventing diabetic and hypertensive retinopathy.
Quit smoking
Smoking creates oxidative stress, damages the retinal vessels and raises the risk of macular disease.
UV protection
UV-protective sunglasses reduce the risk of retinal damage from prolonged sun exposure.
Regular exercise
Physical activity supports circulation and oxygen delivery to the retina and helps control diabetes.
Can disease in the body be seen in the eye?
Yes. The eye is one of the few organs where the body's circulation can be observed directly. A thorough retinal exam can reveal early signs of some systemic diseases.
- Diabetes
- Microaneurysms, haemorrhages and oedema (diabetic retinopathy).
- High blood pressure
- Narrowing, hardening and leakage of vessels (hypertensive retinopathy).
- High cholesterol
- Retinal vascular occlusions and deposits in the vessels.
- Autoimmune disease
- Vessel inflammation (retinal vasculitis) and signs of uveitis.
- Blood disorders, cancer
- Retinal haemorrhages and cotton-wool spots.
- Cardiovascular disease
- Artery occlusions, which can be an early sign of stroke and heart risk.
This is why a regular eye exam is valuable not only for eye health, but for monitoring your general health too.
Frequently asked questions
Is macular disease the same as a retinal disease?
The macula is the small central part of the retina, so macular conditions are one group within the broader family of retinal conditions. Macular disease usually refers to age-related macular degeneration, while retinal disease also covers conditions affecting the rest of the retina, such as diabetic retinopathy or a retinal detachment.
Will my pupils need to be dilated for the exam?
A thorough look at the retina usually needs the pupil widened with drops. For a few hours afterwards your vision can be blurry and your eyes more sensitive to light, so it helps to bring sunglasses and, ideally, to arrange not to drive yourself straight after.
What is OCT, and does it touch the eye?
OCT (optical coherence tomography) is a scan that takes a detailed cross-section of the retina and macula. It does not touch the eye, uses no injection, and takes only a few minutes. It can show subtle changes before they affect your vision.
Will I need injections forever?
Because the effect of intravitreal injections lasts only a limited time, treatment is usually given at regular intervals. It may start monthly; if the response is good, the interval is extended. Some patients need only a few injections, others longer-term treatment; it depends on the type and course of the disease. In higher-risk cases it is important not to miss injections.
How often should I have my retina checked?
It depends on your age, your history, and any existing condition. People with diabetes are generally advised to have a dilated retinal exam at least once a year, and anyone with new symptoms should be seen promptly.
If you have a concern about your vision, or would like to arrange a retinal check, please feel free to get in touch.